

Wow – so it’s now been over 2-months since we ratified our new collective agreement. As you know it was our toughest negotiations yet – taking over 5 months and many long days around the table with Te Whatu Ora.
We had a huge response to the vote with 84.5% of members voting in favour and based on our survey data it meant that 97% of members received a pay rise and 90% received a pay rise of 14% or higher in the first year, with an average of 18% over the 2-year term.
We absolutely recognise that for a small number of members, it did represent a zero-pay increase and where this has occurred, we negotiated an income protection clause. The changes made now mean that the new salary scales can be broken down into an hourly rate that stays the same as RMOs change categories.
In addition to our FAQs that we developed initially, from what we’ve heard from around the ‘water cooler’ chat we thought it was worth re-visiting the detail around some of the most common questions. So, here goes...
How come my pay increase differs to my colleagues? Why was a differential pay deal negotiated?
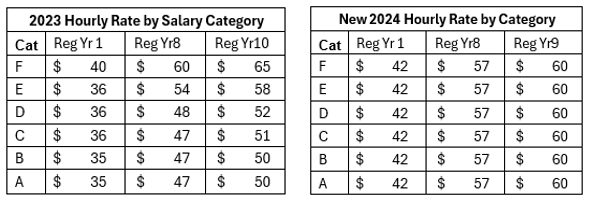
It is important to understand how the pay scales were historically designed, how they have eroded over time and why rebasing is important.
Resetting the scales has demonstrated that over time the lower categories have received an hourly rate that is more than RMOs working higher categories. Meaning for those working longer or more un-social hours, their time was of lesser value.
Rebasing towards an equal hourly rate and implementing a penalty structure therefore unavoidably delivers some RMOs a pay rise and others none.
Due to the overall cost to 'catch up' the hourly rate of the higher categories the lower categories could only be minimally increased.
Also given the hourly rate is multiplied up from the lower categories any increase in the lower categories, further increases the investment required in the higher categories which given the investment already committed, this was unattainable.
Most RMOs work a range of categories over their careers, and so the value of the new agreement will be seen by members earlier on, and throughout their time as an RMO.
It is not easy presenting a differential pay deal, many of our members have been asking for us to re-address the equities in our PayScale since STONZ was first formed, and we believe we have made in-roads towards this in this negotiation. We did ask Te Whatu Ora to consider something for our F category members at the higher end of the scale as part of this deal, but they were unwilling to consider it given the amount of investment that was required to bring the other categories on to a more equal underlying base rate.
Does the STONZ contract favour some specialties over others?
The STONZ deal involved re-basing the salary scales so that RMOs are paid the same hourly rate whether you are category F or category A regardless of your specialty.
It also re introduces a loading so that pay categories which regularly have long days and weekends have penalty payments built in so that when RMOs are giving up their evenings and weekends their hours are being respected.
Whilst re-basing appears to be favourable to some specialties over others, when analysed critically it is simply a mathematically robust approach to pay. The outcome means that hours worked by any RMO are paid fairly.
Won’t compressing the salary scale disadvantage some RMOs?
We believe the compression of the scale will have a positive impact on the overall salary of RMOs across your career - by putting more money in earlier in the scale and by shortening the scale it gets more money to RMOs faster so cumulative income will increase quicker which the team feel is good for everyone including those starting families and paying off mortgages etc.
A long salary scale has pros and cons, and it is important to consider these critically.
The reality is it is the distribution of pay that is the most important part for the finances of the employees. We could have kept step 10, but it would have meant smaller increases each year but when we crunched the numbers, we worked out it was better to stay on say step 9 at a higher salary than have more steps but be drip-fed the increases by the employer.
For those taking parental leave; the annual increments that are in the SECA will remain for those coming through so where someone takes PL, even though they haven't worked for a time, that time away will still be counted towards a salary step.
Loss of a step of a salary does not necessarily mean the workforce is being paid less or missing a pay rise. The quantum of pay lost in the 10th registrar and 4th house officer step has been reinvested in earlier steps and used in the rebasing for antisocial hours as above. Therefore, RMOs have access to this pay earlier and therefore are financially better off rather than being drip fed smaller pay rises over a longer period.
We recognise at STONZ that training and progressing RMOs is taking too long and affecting the pipeline. Reducing the length of the salary scale is in line with our direction that RMOs are selected and progressed in training over a shorter period of time.
Why did you make the changes to Urban/Non-Urban – Rural Scales?
We had to spend a lot of the investment of the offer to 'fix' the hourly rate issue in the salary scale and reinstate antisocial hours which is an issue that affects every single RMO.
We tried hard to negotiate to keep all the prior-listed centres, however with the back and forth that comes with negotiations the argument for those centres to maintain rurality is not as strong as the centres that we have brought into rural loading's. Therefore, some hospitals have gained it, and some have lost it. There is simply not enough money invested to give fair pay to all RMOs for the time they spend in the hospital, to give rural loading's to rural hospital's that need it. That is after the most protracted negotiations STONZ has had so far.
There are mechanisms to get hospitals back on the rural list and a key part of that is through the rural College. We expect the College to lead the way in rural health care in Aotearoa and have armed them with a new financial incentive to best direct to the areas that need it most. We believe they are best placed to analyse rural/difficult to staff data and guide financial investment. We see this as a viable avenue to get centres back on the rural list.
Rurality and hard to staff are ill defined and not necessarily the same, which speaks further to our delegation to the College to guide where this investment goes. Te Whatu Ora is also having a separate conversation regarding hard to staff services and specialties, and we expect more work to occur around this outside of negotiations.
That said - whilst those training and pursuing and prioritising careers in rural health care may not currently be in a hospital recognised by the changes. We expect that over their training careers they will spend significant and more (due to the list adjustment) amounts of time in hospitals with the loading than they did previously.
What’s the importance of Run Reviews following implementation of the new SECA?
It’s crucial to ensure that you have an up to date Run Description which reflect the correct category you are working. Run reviews can be initiated by both parties and Te Whatu Ora are going through a process to ensure that every department has a Run Description.
If you don’t have one, or you believe the category is inaccurate please let in touch with the team.
Also, a reminder that letter/referral writing, result sign off should all be included in clinical time. As and per our SECA Clause's 4.8 & 7.2, Teaching time and admin time should be allowed for and remunerated.
If you want to read more about the changes to remuneration framework you can do so on our website HERE and don’t forget our full list of new SECA FAQs HERE.
STONZ formed in response to a group of RMOs who didn’t feel the rosters and some elements of the collective at the time worked for them. We hope that our new SECA represents what we have heard from members, and that is a significant catch-up on hourly rates that have trended down over the last decade and reconstruction of anti-social hour loading's respecting the long hours done by junior doctors all hours of the day and night.
We had seen RMO pay decline to the point where doctors' hourly pay had fallen below that of nurses. This agreement corrects this to a degree, but it is only a first step.
We advocated that RMOs are the doctors who keep the hospital doors open, we represent about a third of the hospital doctor workforce however we account for two thirds of doctors’ hours worked in Aotearoa New Zealand's hospitals.
We believe that the agreement struck is fair given the current context and the large majority of our members have agreed. However, if we are to grow our workforce and keep it here, more needs to be done. Particularly in terms of improving health infrastructure and growing training opportunities.
Our members have a strong commitment to a better health system and to the New Zealanders it should serve, and that work extends well beyond these pay negotiations. So, we are now getting to work on our ‘projects’ including continuing conversations on how we can further develop the new remuneration model.
If you have any questions, or have heard anything that doesn’t sound quite right – let us know and we’ll de-mystify it 😊